")

This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
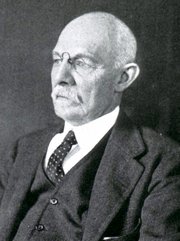
William S. Halsted
mouseover for
Samuel J. Crowe
In my many years working with medical industry, surgeons, and surgery, I have heard many times that such and such surgical technique follows “Halsted’s Rules of Surgery”. The problem is that only two of these “rules” were mentioned and never did I receive an answer while working with Ethicon and Ethicon Endosurgery, and never did I receive an answer as to where could I find the reference regarding the other rules, if they even existed.
I recently read a great 1957 book by Samuel James Crowe, MD (1883-1952), titled “Halsted of John Hopkins; the man and his men”. Dr. Crowe lived for one year with Dr. William Stewart Halsted (1852-1922) and his wife as a medical student at John Hopkins. He was also an intern for Dr. Harvey Cushing, and although he wanted to follow Cushing into neurosurgery, Dr. Halsted placed him in charge of the newly created department of otolaryngology at John Hopkins, a position he did not want. Dr. Crowe went on to become a world-wide renown otolaryngologist.
Here are Halsted’s “Rules of Surgery” as explained by Dr. Crowe, based on Halsted’s research, experiments, and observations (with my own notes and comments):
1. Wounds are resistant to infection when no bits of tissue have been:
a. torn with clamps
b. torn by the rough handling of retractors
c. devitalized by hastily and carelessly applied ligatures
Note: this follows the ancient rule of “Primum Non Nocere”: first and foremost, do not harm
2. Wounds or parts rich in blood vessels usually heal without any visible granulation, even when no antiseptic precautions have been taken.
3. Incisions should be closed carefully and gently, layer by layer
4. The approximating sutures should never put the tissues under tension, since tension interferes with the blood supply and may cause necrosis
Note: Tension-avoidance surgical techniques follow this, one of the prime rules of surgery.
5. The end of the forceps used to pick up bleeding points should be small, to avoid crushing and destroying the vitality of surrounding tissues
Note: This observation led to the creation of fine, multiple toothed thumb forceps used today in cardiovascular surgery , such as the Cooley, DeBakey, Castaneda, etc. type forceps.
6. A drain is essential when there is necrotic tissue and infection
7. Silk should never be used in the presence of infection
Note: This makes sense. Since silk is an organic material, infected tissues will react to the presence of this extraneous material causing more inflammation, and the phagocytic cells in the tissues will destroy the silk and its capacity to hold the tissues together
8. The silk (suture) employed should never be coarser (larger gauge) than necessary and it is well to employ a suture a thread that is not stronger that the tissue it holds
9. A greater number of fine stitches is better than a few coarse ones
Note: This also makes sense. Halsted was known to be extremely meticulous and he could place a hundred stitches of fine silk thread where other surgeons would place a lesser number of coarser stitches. Using a larger number of fine stitches distributes the approximating tension of the sutures over a larger area, thus reducing the chance for suture dehiscence.
10. Avoid when possible the combined use of silk and catgut in a wound
11. For sewing up an abdominal wound, when it is necessary to take heavy deep stitches perforating skin and muscles, silver wire serves admirably
Note: Remember the times when these guiding principles where laid. Nylon, polypropylene, and other synthetic absorbable and non-absorbable sutures had yet to be discovered. Today the same dictum would probably say “For sewing up an abdominal wound, when it is necessary to take heavy deep stitches perforating skin and muscles, a synthetic non-absorbable suture material serves admirably”
It must be noted that Halsted never called the above the “rules of surgery”, rather they are observations that have become guiding principles. These have influenced the world of surgery to this day.
SIDE NOTE: It has been said many times that Dr. Halsted was the first to use rubber gloves. This is not true, Dr. Crowe says that “it was an evolution rather than a happy thought” and it involved his wife Caroline Hampton. This will be the subject of another article.