![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 234 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
- Hits: 294
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
")
Hakaru Hashimoto (1881-1934)
Hakaru Hashimoto, was a Japanese surgeon known world-wide today by the thyroid disease that bears his name… Hashimoto’s disease, a condition which causes goiter and hypothyroidism
Hashimoto was born in the village of Iga, about 30 miles (50km) east of Nara, the first permanent capital of Japan on May 5th, 1881. His family had practiced medicine for generations. He was the son and grandson of physicians.
After graduating from high school in Kyoto in 1903, he decided to study medicine at the Fukuoka Medical College of the Kyushu Imperial University and graduated by 1907. He was invited by his professor of surgery at Fukuoka, Hayari Miyake (1867–1945) to stay. Dr. Hashimoto completed his surgical training in 1912. Interestingly, Dr. Hashimoto did his surgical training while Dr. Sunao Tawara (1873 - 1952), discoverer of the heart's atrioventricular node, was a professor of pathology at the same university. For sure their paths crossed more than once!
During his surgical training Dr. Miyake asked Hashimoto to examine the pathological features of four unusual goiter cases, all women over 40 which had been subject to a partial thyroidectomy. At the time it was thought by some that the disease was an initial stage of Riedel’s(*) thyroiditis, which has far more fibrosis than what we know today as Hashimoto’s disease. Riedel’s thyroiditis also presents with rock-hard thyroid glands which adhere to the surrounding tissues making surgery difficult, which was not the case of these four women.
Dr. Hashimoto noted that the histology of these women was similar to Graves’(**) disease (a type of hyperthyroidism) but that both conditions were clinically different, as some of the four patients were hypothyroid.
An important difference was what he found regarding the common colloid goiters. There was a massive overgrowth of lymphatic elements which, as already stated, were similar to Graves goiters.

Illustration from Hashimoto's 1912 publication
Under the guidance of Professor Miyake he reported his findings and named this condition as “Struma Lymphomatosa” publishing an article in German “Zur Kenntniss der lymphomatosen veränderung der Schilddrüse (Struma lymphomatosa)” [On the lymphomatous change of the thyroid gland (struma lymphomatosa).] in the “Archiv für Klinische Chirurgie” in 1912.
He left Japan for Göttingen University in Germany to study with Professor Kaufman, chairman of the Department of Pathology, and worked on tuberculosis of the urinary tract. He left for London in 1914 after the outbreak of World War I where he studied for another year before returning to Japan.
In 1916 he set up a surgical clinic at his own home and married in 1920. Unfortunately, he contracted typhoid fever while working hard against an outbreak in his district in 1933. Dr. Hashimoto died on January 9. 1934. He was 52 years old.
His discovery opened avenues of research leading to great advances in endocrinology and immunology among others. Hashimoto’s disease was finally recognized as an entity by the end of the 1930’s and the term has been widely used since then.
Personal note: This article was suggested and written by my good friend and classmate Dr. Roberto Villaseca Najarian, an endocrinologist in Santiago, Chile. Dr. Miranda.
Sources:
1. Krustrimoviv, N; Fazzino, GFM; Gallo, D. et al. Dr Hashimoto and the discovery of autoimmune hypothyroidism. (PDF) Medicina Historica 2023; Vol. 7, N. 2: e2023034 9
2. Sawin, Clark T. M.D. Hakaru Hashimoto (1881–1934) and His Disease. The Endocrinologist 11(2):p 73-76, March 2001
3. Hashimoto, H. Zur Kenntniss der lymphomatosen veränderung der Schilddrüse (Struma lymphomatosa) Archiv für Klinische Chirurgie, 1912 (PDF)
4. Hashimoto, K. Life and Times: Hakaru Hashimoto. ThyroWorld Spring 2006:16. (PDF)
Notes:
(*) Bernhard Moritz Carl Ludwig Riedel (1846-1916) German surgeon.
(**) Robert James Graves (1796 – 1853) Irish surgeon.
Dr. Hashimoto's portrait, public domain, enhanced via AI
- Details
- Written by: Efrain A. Miranda, Ph.D.
In 1543 Andreas Vesalius was staying at the city of Basel, in Switzerland. The reason for his visit was to oversee the preparation and printing of the first edition of his opus magnum, a book titled ”De Humani Corporis Fabrica, Libri Septem” (Seven Books on the Structure of the Human Body). This book , colloquially known as the “Fabrica”, would change the history of anatomy and become the beginning of scientific, fact-based description of the human body.
The other individual in this story was Jakob Karrer Von Getweiler, a notorious bigamous criminal who lived in Basel. Jakob attacked and stabbed his wife when she confronted him because she found that he had a second wife. Although seriously injured, she survived, but Jakob Karrer was sentenced to death by beheading, a current sentence at the time. The sentence was carried on May 12th, 1543.
 Andreas Vesalius
Andreas Vesalius

Jakob Karrer Von Getweiler
Because of the laws regarding human dissection (also called anatomizing), only the bodies of executed criminals were permitted to be used as teaching specimens. The dissection was public and anyone, alongside medical students, was permitted to attend. In fact, it was considered public entertainment. Most probably the town council, having a famous anatomist such as Vesalius in town, offered him the opportunity for this public dissection. The title page of the 1555 Fabrica shows this "circus" of a public anatomy with Andreas Vesalius at the center.

1555 Fabrica Title Page
After the dissection, Vesalius proceeded to clean, boil, and dry the bones and, following the instructions in his own book (Book one, Chapter 39), mounted the bones as an anatomical exhibition. Little did Vesalius know that 483 years later, that skeleton would still be in existence and carry the fame of being the oldest anatomical specimen in the world.
Here is the video for the first part of this article.
Additional information found in the Fabrica.

Click for a larger image
Chapter 39 of the Fabrica is extensive and lists in detail how to dissect and clean the bones. One technique is shown in a historiated initial wood block. These were placed at the beginning of chapters. In this case it is the letter “C” of the 1543 Fabrica. The illustration shows three individuals placing the dissected body in a river in a wooden perforated box so that the bones slowly macerated to make it easy to clean all organic matter later.
The next historiated initial is the letter “slanted O” of the 1543 Fabrica. In this image you can see two individuals bringing a head down the gallows while a child holds a basket for the head. This was a preferred technique to study the head without the putrefaction of the rest of the body. The 1555 second edition initial is different, but with the same motif.

1543 edition historiated wood block

1555 edition historiated wood block
The third initial is the “O” in the 1555 Fabrica. This is an important representation using putti. These were images of chubby children, sometimes with wings, common in medieval and renaissance imagery. In this letter we see 5 putti, one of them holding a bone, another tending to the fire under a cauldron and one placing a skull in the boiling water.


1955 Vesalius bone drill design
In the 1555 second edition of Fabrica, Vesalius added an illustration of a bone drill of his own design, which can be seen here.
In 2023, with the occasion of the Vesalius Triennial Meeting in Antwerp, my friend Dr. Randall K. Wolf and I visited Dr. Francis Van Glabeek, an orthopedic surgeon from Antwerp and an enthusiast of Vesaliana.
We discovered that in 2018 Dr. Van Glabeek had built the bone drill following Vesalius instructions! With my friend Dr. Randall K. Wolf, we were able to operate this drill, that to my understanding is the only one in the world.

Dr. Francis Van Glabeek demonstrating Vesalius' bone drill
Here is the video for the second part of this article.
Sources:
1. "A Bio-blibliography of Andreas Vesalius" Cushing, H. 1943 Saunders
2. Francis Van Glaabek “Une reconstruction du trepan a arc d’André Vésale” 2020 Carnet d’histoire de la Medicine
3. Daniel H. Garrison, Ph.D.; Malcolm Hast MD. "Andrea Vesalius: The Fabric of the Human Body, An Annotated Translation of the 1543 and 1555 Editions of “De Humani Corporis Fabrica Libri Septem". Volume 1/2"; ISBN: 9783318022469 Basel: Karger, A.G., 2014.
4. Lambert, Samuels "Three Vesalian Essays to Accompany the Iconaes Anatomicae of 1934"; New York: MacMillan, 1952.
Note: Image of the skeleton of Jakob Karrer Von Getweiler. Public domain. Amada44, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
- Details
- Written by: Efrain A. Miranda, Ph.D.

Dr. José Manuel Revuelta
Personal Note: Through my good friend Tito Estrada, I read an very interesting article in Spanish by Dr. Jose Manuel Revuelta. Dr. Revuelta is a Professor of Surgery and Professor Emeritus at the University of Cantabria. Former Head of Cardiovascular Surgery at Valdecilla Hospital in Santander, Spain. Dr. Revuelta contributed the article on "The Little Brain Inside the Heart" which we published in 2025.
The article's title (in Spanish) is "La ingeniería invisible que nos mantiene vivos" (The invisible engineering that keeps us alive), the incredible activity of the cardiac cells and the anatomical description of a helical heart muscle pioneered by Dr. Francisco Torrent-Guasp (1931 - 2005).
He has graciously granted us permission to translate and publish his article in “Medical Terminology Daily”. Dr. Miranda.
The Invisible Engineering That Keeps Us Alive
José Manuel Revuelta Soba
We are talking about a self-exciting, autonomous electrical system, a precision biochemical engine, a power plant capable of changing its "fuel" on the fly to power a very peculiar muscular architecture.
Millennium after millennium, humankind has gazed in awe at this constant pulse that marks the rhythm of life. When we try to repeatedly clench and unclench our fist tightly, in just a few minutes, the fatigue in our forearm forces us to stop. However, just inches away, a muscle the size of that fist contracts rhythmically 100,000 times a day without stopping. For the heart, muscle fatigue is not an option.
How does this organ manage to defy the laws of wear and tear that govern the rest of our biology? There is no man-made engine capable of withstanding such a level of friction and mechanical stress without external maintenance for eight or nine decades. Maintaining that uninterrupted heartbeat is no trivial feat; it's the result of a masterpiece of natural engineering. We're talking about an autonomous, self-exciting electrical system, a precision biochemical engine, a power plant capable of changing its "fuel" on the fly to power a unique muscular architecture.
The Engine That Generates Its Own Electricity
This marvel of endurance begins with an astonishing phenomenon: the heart doesn't wait for orders; it commands itself. Unlike the rest of our muscles, which depend on instructions from the brain, the heart contains a self-sufficient power plant.

Sodium-Potassium Pump
The secret of this "miracle" lies in a coordinated exchange of minerals. Through microscopic gates located on the surface of the heart cells (ion channels), sodium and potassium ions rhythmically enter and exit. This flow, known as the sodium-potassium pump, creates an electrical potential difference. The result is tiny millivolt discharges that travel through the organ like a controlled shock wave. Each of these impulses—normally between 70 and 80 per minute—propagates through a network of specialized cardiac cells that function like the wiring in a building. This current is what the electrodes of an electrocardiogram (ECG) capture, mapping the activity of our internal "electrical network" on paper.
What is truly remarkable about the heart's electrical system is its redundancy. The main generator (sinoatrial node) sets the pace, but if it fails, the system doesn't shut down; immediately, another backup generator (atrioventricular node) kicks in, capable of activating in milliseconds to maintain the heartbeat. This energy is transmitted through an intracardiac conduction network until it reaches the Purkinje network, the final stretch of wires that makes the muscle contract and keeps life going.
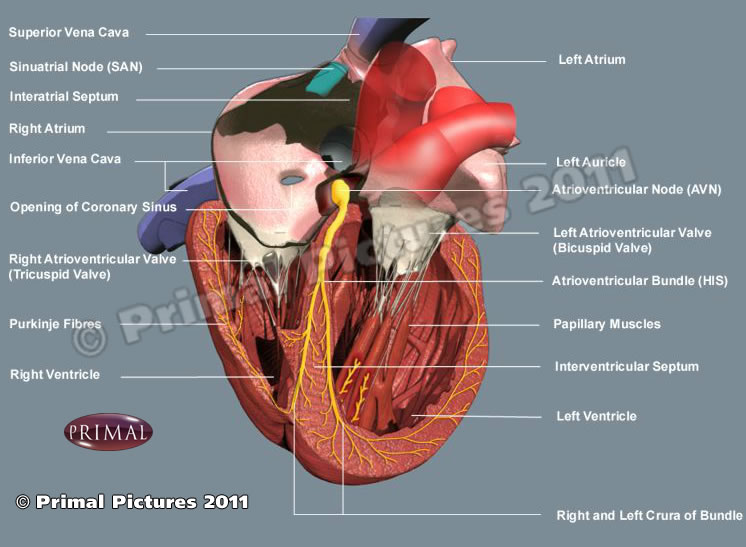
Conduction system of the heart
Amazing Biochemical Engine
If the electrical system generates the spark for ignition, calcium is the inductor that generates the movement. For the heart to contract with the force necessary to pump blood throughout the body, its cells must be flooded with this mineral at high speed. However, managing this flow is not simple: it requires precise biological engineering.
Within the heart cell, there is a specialized reservoir called the sarcoplasmic reticulum. Its function is to store, release, and recover calcium in fractions of a second. It is a closed-loop recycling system that ensures nothing is wasted and that the engine is always ready for the next cycle. When the electrical impulse arrives, ultrasensitive gates burst open, and calcium is released, activating the proteins that trigger contraction (systole). But for the heart to relax and refill with blood (diastole), that calcium must disappear immediately. This is when SERCA (sarcoplasmic/endoplasmic reticulum Ca2+-ATPase) proteins come into play. These proteins act as powerful suction pumps and, in a matter of milliseconds, draw calcium back into the sarcoplasmic reticulum, leaving the muscle relaxed and ready for the next movement.
This cycle of calcium delivery and retrieval occurs about 70 times per minute, but during intense exertion, the system can accelerate to more than 180 cycles per minute without losing synchronization. This ability to manage calcium so quickly and efficiently is what prevents the heart from cramping or becoming fatigued, as happens to our leg muscles after a strenuous run. While other engines might overheat or seize up, the heart uses this perfect recycling cycle to keep running.
A High-Performance Power Plant
If calcium is the messenger of contraction, mitochondria are the boiler that keeps the entire system running. In a typical muscle, mitochondria occupy barely 5% of the cell volume, while in the heart they constitute 35%. They are strategically located on the surface of the cardiac muscle fibers (cardiomyocytes) so that energy transport is practically instantaneous. Unlike other organs that store energy for later, “the heart lives for the day”; it produces and consumes its fuel, a molecule called ATP (adenosine triphosphate), in intervals of 8 to 10 seconds. To move this fuel from the mitochondria, the heart uses phosphocreatine, an ultrafast transport vehicle that guarantees a continuous and uninterrupted flow of energy.
While muscles can work briefly without oxygen—generating lactic acid, responsible for muscle soreness—the heart is an “oxygen addict.” Its metabolism is purely aerobic, allowing it to extract energy from every molecule. The most surprising aspect of this engineering is its flexibility; while the brain only accepts oxygen and glucose, the heart is an “efficient omnivore.” Its preferred fuel is fatty acids, but if the situation demands it, it can burn glucose or even lactate. This ability to switch fuels, depending on availability, ensures that the cell powerhouse (mitochondria) never runs out of supply, whether due to prolonged fasting or intense stress. In short, a perfect balance between energy production and expenditure without any rest.
The Helical Muscular Architecture
For decades, it was believed that the heart was a simple muscular sac that inflated and deflated autonomously. However, thanks to the pioneering vision of the Valencian (from Valencia, Spain) cardiologist Francisco Torrent-Guasp (1931 -2005), we now know that cardiac anatomy is much more sophisticated: the heart is a unique muscular band that coils upon itself in a spiral shape.
To understand how it works, let's forget the idea of a balloon being compressed. Instead, think of a wet towel we want to wring out: we don't press it from the sides, but rather twist it. The heart's engineering follows precisely this principle; its fibers are arranged in a spiral. During systole, the heart rotates on its own axis, performing a "corkscrew" motion. This rotation allows it to expel blood with a force and hemodynamic efficiency that a simple radial contraction could never achieve. But the most ingenious thing happens right at the end of the heartbeat: the elastic unwinding of this muscular band generates a vacuum effect that draws the blood back in. Instead of expending extra energy to fill up, the heart uses its own elastic architecture, it's energy efficiency in its purest form.
In this video, Dr, Torrent-Guasp demonstrates the helical architecture of the musculature of the human heart
Torrent-Guasp spent decades analyzing the hearts of various species in his small home laboratory in Denia, ignored by the scientific community. His luck changed when the prestigious surgeon Gerald Buckberg, from the University of California, Los Angeles (UCLA), recognized the brilliance of his discovery. Buckberg not only disseminated this theory internationally, but also designed a ventricular remodeling surgical technique, which he named "Pacopexy" in honor of his friend Paco Torrent. (Paco is the Spanish nickname for Francisco)
Currently, Torrent-Guasp's concept of the myocardial muscular band is studied at the world's leading universities. It is definitive proof that the heart is not just a muscle, but a marvel of human biology; a continuous muscular structure, without attachment points or independent elements that can fail, designed to adapt to changing hemodynamic pressures throughout a lifetime.
The true genius of the heart's invisible engineering lies not only in its electrical power or its elegant helical geometry, but in a capacity that any engineer would envy: constant self-repair while fully functioning. At the molecular level, proteins damaged by the uninterrupted effort are replaced by new copies without the rhythm being altered in the slightest. It is a unique resilience; we could say that "the heart never rests because it never stops renewing itself."
Ultimately, this organ is a testament to a brilliant biological technology that has perfected the art of enduring, a machine that refuses to surrender to fatigue. Each heartbeat is not just a movement; it is the triumph of the heart's biological engineering.
"What lies behind us and what lies before us are small things
compared with what lives within us"
Ralph Waldo Emerson (1803-1882)
American philosopher and poet.
Notes: The Sodium-potassium pump image public domain, courtesy of Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine (2). DOI:10.15347/wjm/2014.010 ISSN. 2002-4436. Derivative by Mikael Häggström
Resources:
1. Bers, D. Cardiac excitation–contraction coupling. Nature 415, 198–205 (2002).
2. Mora, Vicente, Roldán, Ildefonso, Saurí, Assumpció, Fernández-Galera, Rubén, Monteagudo, Marta, Romero, Elena, Cabadés, Claudia, Cosín, Juan A., Trainini, Jorge C., & Lowenstein, Jorge A. Correspondencia de la deformación miocárdica con la teoría de Torrent-Guasp. Aporte de nuevos parámetros ecocardiográficos. Revista argentina de cardiología, 84(6), 1-2.
3. Website of Dr. Torrent-Guasp and family
4. Buckberg, G., Hoffman, J., Mahajan, A., Saleh S., Coghlan, C. Cardiac Mechanics Revisited: The Relationship of Cardiac Architecture to Ventricular Function. Circulation 118, 24
5. Buckberg G, Mahajan A, Saleh S. Structure and function relationships of the helical ventricular myocardial band. J Thorac Cardiovasc Surg, 2008; 136, 578-589.e11
6. The following 37 minute video was published in 2005 features Dr. Torrent-Guasp and is available on YouTube:
- Details
- Written by: Efrain A. Miranda, Ph.D.
One of my interests is the origin and evolution (etymology) of medical terminology. Because of this, in October 2012 we started on the Clinical Anatomy Associates website a blog called "Medical Terminology Daily". Originally, I thought we could do one article per day… oh how wrong I was!!, but we kept the name and, since then, over one thousand articles have been published.
The first article in the blog was the medical term “Bariatric”. Today we will analyze this term again and the medical derivations that arise from one of these root terms.
The term "bariatric" is a compound word with two Greek roots: βάρος, meaning "weight" or "pressure", and γιατρός meaning "doctor, physician, or healer". The adjectival suffix [-ic] that closes the word means "pertaining to". The term bariatric then means "pertaining to weight-related medicine".
Let’s look at some of the many uses of the root “iatr-“in medical terminology. Remember, you only add an “o” as in “iatr-o” (the combining form of a word) when you are combining a root term with another root or a suffix.
TERM
ETYMOLOGY
(in addition to iatr-)
DEFINITION
Iatrogenic
synonym (nosocomial)
Greek: γέννα (génna) meaning birth, create, produce
Denoting an illness or adverse condition caused by medical treatment or physician intervention
Pediatrics
Greek: παιδί (paidí) meaning child
The branch of medicine dealing with the health and medical care of infants, children, and adolescents
Psychiatry
Greek: ψυχή (psychí) meaning mind/soul
The branch of medicine focused on the diagnosis, treatment, and prevention of mental, emotional, and behavioral disorders
Geriatrics
Greek: γέρος(géros) meaning old.
The branch of medicine dealing with the health and care of old people
Podiatry
Greek: πόδι (pódi) meaning foot
The branch of health care dedicated to the study, diagnosis, and treatment of disorders of the foot
There are variations of the suffixes added to the root term iatr-. Examples of these are:
-iatry - denoting the field of practice, such as pediatry, podiatry, psychiatry. etc.
-iatrist - the person practicing that particular field, such as psychiatrist, geriatrist, etc.
-iatrician - another way of denoting the field of practice, such as pediatrician.
- Details
- Written by: Efrain A. Miranda, Ph.D.
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
")
In late March 2026, I was reading an article on the Journal of Clinical Anatomy written by R. Shane Tubbs PhD. MS, PA-C, past president of the American Association of Clinical Anatomists. The article was titled “Doctors Without Anatomy Are Like Moles: They Work in the Dark…”.
He was referring to a dictum by Friedrich Tiedeman, MD. His original dictum was:
“Ärzte ohne Anatomie gleichen Maulwürfen: sie arbeiten im Dunkeln, und ihrer Hände Tagewerk sind — Erdhügel”
The translation is in the first image in this post. Dr. Tubbs journal article led me to research Tiedemann’s life, scientific work, and legacy, where besides his famous sentence (which is very common use in Germany medical schools) I found a correlation between Tiedemann' work and a famous energy drink!
Friedrich Tiedemann (1781–1861) was a German physician, anatomist, physiologist, and zoologist. Born in Kassel, Germany. He studied medicine at the University of Marburg, where he graduated with an MD in 1804. Soon after graduation he abandoned medical practice and dedicated himself to scientific research and academic teaching, focusing particularly on anatomy and physiology.
At the University of Marburg, he taught physiology and comparative osteology. In 1805, at only twenty-four years of age, he was appointed Professor of Zoology, Human Anatomy, and Comparative Anatomy at the University of Landshut.
Later, in 1816 he took the chair of anatomy and physiology at the University of Heidelberg until his retirement in 1854. During these three decades he served as director of the anatomical institute, including various university administrative roles including dean and prorector. He took retirement because of increasing blindness, and he was forced to sell his library which contained thousands of books,
During his tenure he expanded the anatomical collections substantially. By the time of his retirement in 1849, the institute contained more than 2,000 anatomical and pathological specimens, including injected vascular preparations and comparative zoological material used for teaching and research.
Tiedemann was elected to several scientific societies, including:
• Royal Society of London
• Royal Swedish Academy of Sciences
• American Academy of Arts and Sciences
• Royal Society of Edinburgh
Tiedemann’s early research focused on the development and comparative structure of the brain. His work "Anatomie und Bildungsgeschichte des Gehirns im Foetus des Menschen" (Anatomy and developmental history of the brain in the human fetus ), published in 1816., examined embryonic brain development and compared human brain structures with those of animals, providing insights into morphological development.
He authored several publications, but probably the most famous was his work “Tabulae Arteriarum Corporis Humani” (Plates of the arteries of the human body) published in 1822 with illustrations by Jacob Wilhelm Christian Roux is a folio-size anatomical atlas devoted entirely to the arterial system. The atlas has 38 large lithographic plates, many originally hand-colored, making it one of the earliest works devoted exclusively to the arteries of the human body. This book is in two different volumes, one with the images (available here) and one with the listing of the structures in both Latin and German (available here)


He was one of the first to challenge racial anthropology, arguing with scientific facts, that social inequalities were products of historical and political circumstances, including slavery, rather than biological differences. Among Tiedemann’s most historically notable publications was “On the Brain of the Negro, Compared with That of the European and the Orang-Outang” (1836–1837)", published in the Philosophical Transactions of the Royal Society.
An interesting side of Tiedemann’s research was the result of his research on the physiology of digestion. In collaboration with the chemist Leopold Gmelin (1788–1853), Tiedemann conducted experimental studies on digestion and metabolism. Their work “Die Verdauung nach Versuchen" (Experiments on Digestion- published on 1827) examined the physiological mechanisms of digestion and helped confirm the role of chemical processes in gastric activity. They analyzed the composition of bile in the bull (Lat: Taurus) and discovered one of its main components (2-aminoethanesulfonic acid) which they called “Taurine” a word derived from the Latin "taurus" meaning bull, because it was discovered in the bull gallbladder and intestine.
Although not an essential dietary component, this compound is used today as a dietary supplement and, believe it or not, it is one of the components of an energy drink … Red Bull! Talk about coincidences!
Sources:
1. Tubbs, R.S. (2026), Doctors Without Anatomy Are Like Moles: They Work in the Dark…. Clinical Anatomy
2. LaTourelle J. Friedrich Tiedemann (1781–1861). Embryo Project Encyclopedia. Arizona State University; 2015.
3. University of Heidelberg Library. Friedrich Tiedemann (1781–1861) digital collections overview. (ub.uni-heidelberg.de)
4. Encyclopaedia Britannica (9th ed.). Tiedemann, Friedrich.
5. Heirs of Hippocrates Collection, University of Iowa Libraries. Tabulae arteriarum corporis humani bibliographic record.
6. Encyclopedia.com. Tiedemann, Friedrich (1781–1861).
7. Royal Society. Friedrich Tiedemann—Fellowship record.
Image of Dr. Tiedemann public domain, AI enhanced for color. Images of Tiedemann's book public domain.
- Details
- Written by: Efrain A. Miranda, Ph.D.
- Hits: 6238
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.
")
K.F. Wenckebach
Karel Frederik Wenckebach (1864–1940) Dutch physician and anatomist born in 1864, in The Hague, Netherlands. Wenckebach enrolled at the University of Utrecht’s School of Medicine, obtaining his degree in 1888.
While at medical school, he developed interest in physiological research, training in laboratory techniques and cardiac rhythm analysis under the mentorship of physiologist Theodor Wilhelm Engelmann (1843 -1909). His early work focused on embryology and rhythm disturbances observed in isolated frog hearts—a critical foundation for his later discoveries in human cardiac conduction and cardiac arrhythmias.
After graduation, Wenckebach briefly practiced medicine in rural Netherlands, where he encountered patients with irregular heartbeats. Through careful observational analysis of arterial pulse tracings—without the benefit of electrocardiographs—he identified a pattern of progressive prolongation in pulse intervals followed by a “dropped beat.” In 1899, he described this arrhythmic sequence, initially termed "Luciani periods", that later came to be recognized as second-degree atrioventricular (AV) block, Mobitz type I, or the Wenckebach phenomenon.
The pattern of this arrhythmia reflected a progressive delay in conduction through the AV node until one impulse failed to be conducted, resetting the cycle. Wenckebach’s work provided early evidence that conduction properties intrinsic to the myocardium and its specialized tissues underlay certain rhythm disturbances rather than ectopic beats alone.

Wenckebach’s insight was notable for preceding the advent of clinical electrocardiography and the anatomical identification of the sinoatrial (SA) node and the atrioventricular (AV) node by Tawara, Keith and Flack and other researchers in the early 20th century.
In addition to describing rhythm phenomena, Wenckebach contributed to early understanding of internodal conduction pathways. In his later work, he described an anatomical tract—now referred to as Wenckebach’s bundle or the middle internodal tract—as part of the internodal conduction system that links the SA node to the AV node.
Wenckebach’s academic career included professorships at the University of Groningen (1901), University of Strasbourg (1911–1914), and University of Vienna (1914–1929). He authored influential texts including Die Arhythmie als Ausdruck bestimmter Funktionsstörungen des Herzens (1903) and Die unregelmässige Herztätigkeit und ihre klinische Bedeutung (1914), which integrated clinical observations with physiological concepts. Wenckebach also investigated pharmacological interventions in arrhythmia, notably promoting the use of quinine for paroxysmal atrial fibrillation.
His contributions earned numerous honors, including honorary fellowships and international recognition. Wenckebach retired in 1929 and continued to study cardiac physiology, including investigations on heart failure in the Dutch East Indies. He died in Vienna on November 11, 1940.
Dr. A.R. Perez-Riera (Brazil) quotes Wenckeback as follows:
“In medical science there are vast realms of which I have no special knowledge and, again, no, I am not a great man; I am a happy man.”
Sources and references:
1. Wenckebach KF. Die Arhythmie als Ausdruck bestimmter Funktionsstörungen des Herzens. Leipzig: Verlag; 1903.
2. Upshaw CB Jr. The Wenckebach phenomenon: a salute and comment on the centennial of its original description. Ann Intern Med. 1999;131(8):634. PubMed PMID: 9890852.
3. Mendoza-Davila N, Varon J. Resuscitation great. Karel Wenckebach: the story behind the block. Resuscitation. 2008;79(2):189-192.
4. Cadogan M. Karel Frederick Wenckebach. LITFL Medical Eponym Library. 2025.
5. Pérez-Riera AR, et al. Median bundle of Wenckebach and internodal conduction pathways in cardiac anatomy. Via Medica (PDF).
6. Zhao Y, Wan J, Liao B, Qi M. The Neglected Internodal Tract-A Cardiac Conduction System Structure Homologous to the Development and Regulation of the Sinoatrial Node. Rev Cardiovasc Med. 2025 Apr 22;26(4):27882. doi: 10.31083/RCM27882. PMID: 40351691; PMCID: PMC12059794.
7. José L. Fresquet. Karel Frederik Wenckebach (1868-1940) Instituto de Historia de la Ciencia y Documentación (Universidad de Valencia-CSIC). Marzo, 2010.
Image of Dr. Wenckebach public domain, AI enhanced for color.