![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 526 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
2017 AACA Meeting – Thursday, July 20
This is the 2017 Meeting of the American Association of Clinical Anatomists (AACA) in Minneapolis, MN. This 34th meeting of the association, gets together over 300 clinical anatomists, anatomists, physicians, and students from all over the world.
Last day of the meeting! In the morning, there was a poster session and a platform session dedicated to the neck and lower limb. Now, I must confess that as much as I wanted to attend the meeting, I decided to go somewhere else and skip the morning session… I should feel bad about this, but I do not!!
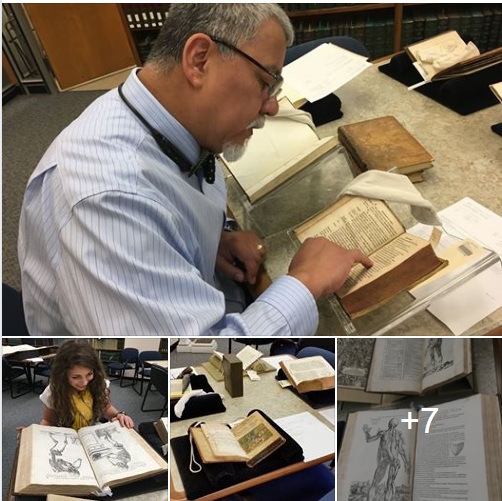
With two other attendees to the AACA meeting I went to the Wangensteen Historical Library which has a collection of over 80,000 rare books. We met with the Curator, Lois Hendrickson, Christopher Herzberg, and Emily Beck.
First, we visited the current exhibit, “Medical Exchanges: Mapping the Human Body in Japan and China” with incredible books, medical posters, and artifacts referencing anatomy, surgery, acupuncture, botanical remedies, etc. Then we went into the reading room where they already had a display of books on anatomy, surgery, histology, etc.
We spent at least four hours reading and admiring these books and the knowledge they contain. One of our discussions was on the fact that today there is a great deal of information “lost” in these books because they have not been digitized, or because many are written in languages which the average researched does not master.
For those who read this blog, you know that I am collector of antique medical books and the opportunity to be at this incredible library was unique. There were so many books that is difficult to list. Authors like Bidloo, Hooke, Verhayen, Mascagni, Vesalius, etc. Books like “De Muto Cordis”, “Micrographia”, “De Humani Corporis Fabrica, Libri Septem”, and “De Humani Corporis Fabrica, Epitome” are some of the jewels that we were able to admire.
Personally, the opportunity to spend time with these books was invaluable. There are only 13 known “De Humani Corporis Fabrica, Epitome” books in the world. It is priceless and who knows what its monetary value would be if any makes it to the antiquarian market. Being able to read, admire and touch this book was the “epitome” of my time at the library (pun intended).
Unfortunately, for some unknown reason I lost all the pictures I took of this occasion, so I hope to get some from the colleagues that went to the library with me.
Back at the AACA Meeting, we had a Medical Terminology Committee meeting, followed by the AACA Business Meeting, and then the closing banquet with the presentation of Awards. The last order of business was the presidential transition. Neil Norton, PhD ended his presidential tenure with the closing of the 2017 AACA Meeting and Marios Loukas, MD, PhD begins his two-year as President of the AACA.
Next year the AACA meeting will be in Atlanta! See you there!
- Details
2017 AACA Meeting – Wednesday, July 19.
This is the 2017 Meeting of the American Association of Clinical Anatomists in Minneapolis, MN. This 34th meeting of the association, gets together over 300 clinical anatomists, anatomists, physicians, and students from all over the world.
Second day of the meeting, by now I have met most all my old friends from the AACA, and I have started making some new ones… I really like this meeting.
The meeting started with the poster session where I am a judge. I made it a point to look at all the posters yesterday and the quality of the presentations is impressive. I am humbled to have to judge so much talent and feel that many deserve the award for the best poster presentation.
The platform sessions for the day were dedicated to the Upper Limb and Education.
There was a special session dedicated to the topic “The Legal and Ethic Consideration of Being the Guardian of the Gift”. This session dealt with the legal and ethical implications of curating and keeping old collections of fetal tissue, osteology, teratology, and anatomical specimens.
I also attended the Clinical Anatomy Terminology Committee meeting… it was fun. We formed groups and tried to make anatomical definitions according to new standards being developed by the AACA.
The day ended with a social event (food and drinks) where we were treated to samples of books from the Wangensteen library (NO TOUCHING) and medical devices from the Bakken museum. What a day!!!
More nice stuff tomorrow!!!

- Details
2017 AACA Meeting – Tuesday, July 18.
This is the 2017 Meeting of the American Association of Clinical Anatomists in Minneapolis, MN. This 34th meeting of the association, gets together over 300 clinical anatomists, anatomists, physicians, and students from all over the world.
The meeting started with the official welcome by the president of the AACA, Neil S. Norton, Ph. D., and the welcome by our local Minnesota host Tucker W. LeBien, Ph.D.
Unfortunately, our Honored Member James D. Collins, M.D., is sick and could not attend. We all wish him well.
The rest of the day was spent in poster sessions, the Tech Fair, and a reception where new AACA members can meet our mentors and possibly connect throughout their careers. The AACA aims to help its members through these activities.
We also had time to visit the exhibit hall where our sponsors can present their products. We sincerely thank them for their contribution.
One of the presentations that caught my attention was the use of augmented reality in anatomy, where you can see an anatomical structure floating in the air superimposed on the environment. 3D anatomical resources were also presented by the exhibitors.
One of the highlights of my day was to meet again with Victor M. Spitzer, Ph.D., (Honored Member AACA 2014) and talk about meeting in Colorado at his lab, and the incredible revolution in anatomy that he started with The Visual Human Project. I invited him to become a contributor to our blog…. Hope he accepts!
The day ended with some of the attendees to the meeting going to see a New York Yankees vs, the Minnesota Twins baseball game…. I stayed. Unfortunately for our hosts the NYY won 6-3.
More nice stuff tomorrow!!!

- Details
2017 AACA Meeting – Monday, July 17.
This is the 2017 Meeting of the American Association of Clinical Anatomists in Minneapolis, MN. This 34th meeting of the association, gets together over 300 clinical anatomists, anatomists, physicians, and students from all over the world.
We started with a judge’s meeting. I will be one of many judges that will evaluate the many posters presented by mostly new AACA members and students sponsored by an AACA member. This is a very important activity, as the winner will be presented with an award. Each poster presenter will explain their scientific research and answer questions from the judges.
After the judge’s meeting, it is time for the inaugural reception. This is the time to meet with old friends and colleagues as well as an opportunity to welcome first time attendees and new AACA members. Luckily, they are easily identifiable by a green badge.
I am very lucky to be here, and looking forward to tomorrow with the inaugural session, the tech fairs, posters sessions, and platform session on the torso.
The following post and pictures will take you to the Facebook page of Clinical Anatomy Associates, Inc.

- Details
This is the first time I embed a Facebook article from https://www.facebook.com/CAAInc.
During this week, I will be attending the 2017 Meeting of the American Association of Clinical Anatomists in Minneapolis, MN. This 34th meeting of the association, gets together over 300 clinical anatomists, anatomists, physicians, and students from all over the world.
I will try to post pictures, and excerpts from some of the lectures, presentations and posters. After the meeting, there will be a postgraduate course which I will also attend.
The meeting will be held at the Minneapolis Marriott City Center Convention Center and is hosted by the University of Minnesota Medical School.
So, let’s start with travel! I flew N21315 to Minneapolis. The flight was IFR, uneventful, at 12,000 ft. (with oxygen support) and landed at KSTP (St. Paul Downtown airport). I decided to post some pictures of the flight and the airplane.
Now I am getting ready for the judge’s meeting and then the reception. I will be posting some pictures tomorrow!

- Details
Cover of the book by Theo Dirix
We are getting closer and closer to the objective, that is, to fund and find the lost grave of Andreas Vesalius, recognized worldwide as the Father of Modern Anatomy. We are setting up the dates for the next phase and preparing the logistics for the crews from Crete and Belgium.
The quest for the lost grave of Andreas Vesalius continues, the permits have been obtained, and we only have the last hurdle to finish, the funding of the project trough our GoFundMe page.
Theo Dirix, a contributor to Medical Terminology Daily, now has an offer that you may like. He wrote the book "In Search of Andreas Vesalius" which relates the beginning of this Quest. The book is out-of-print today, but there are a few copies available. By donating 30 € (US$35)you'll receive one of the last available copies and you'll be mentioned in the sequel of the book that will be dedicated to the next stage of the project.
The project is private and funded by those who believe we still have an opportunity to find the lost grave. For more information, you are welcome to read Theo Dirix's article : "To put it in another way: where do we have to look for Vesalius's grave?"
Here are some reviews for Theo Drix's book "In Search of Andreas Vesalius" :
Vivian Nutton: "I read with pleasure and wry amusement Theo’s account (..) and was reminded of reading the autobiographical account by Stephen Miller of his time as head of the American archaeological school and the boss of the Nemea excavations in the 1980s and 90s (...)
(Professor Vivian Nutton specialises in the history of the classical tradition in medicine, from Antiquity to the present, and particularly on Galen, some of whose works he has edited and translated, and on medicine during the Renaissance.)
Jacqueline Vons: " here is a book " without claim " but well documented, which is committed to tracing the research made to zakynthos by the author and a team of doctors, historians and artists to find the tomb of vesalius (1514-1564).
(Jacqueline Vons est professeur agrégé de lettres classiques, docteur ès études latines, enseignant-chercheur habilité à diriger des recherches. Elle a enseigné le latin et l'histoire de la médecine au CESR et à la faculté de Lettres de Tours et a assuré pendant plusieurs années des enseignements complémentaires en sciences humaines à la faculté de Médecine. Ses thèmes de recherche sont orientés vers l'histoire de la médecine et notamment autour d'André Vésale (éditions, traductions, transcriptions), de la pensée et des pratiques médicales en France à l'époque moderne ainsi que des textes médicaux latins centrés principalement sur l'anatomie.)
Maurits Biesbrouck: in search of Andreas Vesalius is so well researched and written, that if the further search for his grave completely shutting down (something we hope not! ) and only after a few decades be rebooted again, the perfect future researchers would know to where you came, and the wire without wasting time we can again. It is a very detailed history of the search that has already been made, a solid status and simultaneously present an extremely valuable tool for further extrapolating.
(Dr. Maurits Biesbrouck has a lifelong interest in Andreas Vesalius. He translated the first book of the De Humani Corporis Fabrica Libri Septem into Dutch, compiled an annually updated Vesalius-bibliography and wrote many articles on his life and works, many as a co-author with Omer Steeno (Leuven, Belgium) and Theodoor Goddeeris (Kortrijk, Belgium). See www.andreasvesalius.be.)
UPDATE: April 25, 2018. Theo Dirix's new book is already published, the names of the contributors have been incorporated in the book. The title of the new book is "In Search of Andreas Vesalius The Quest for the Grave, Lost and not yet found". Dr. Miranda