![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 1029 guests and no members online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
- Written by: Coninx, R; Dirix, T
Did Andreas Vesalius really die from scurvy on the island of Zakynthos in 1564?
Evidence does not support this theory.
NOTE: The following article authored by Theo Dirix, and Dr. Rudi Coninx, is a rebuttal of Pavlos Plessas' theory that Andreas Vesalius indeed died from scurvy. The original article entitled "Powerful indications that Vesalius died from scurvy" by Pavlos Plessas was presented in a meeting at the island of Zakynthos in 2014.

Dr. Rudi Coninx, and Theo Dirix
Andreas Vesalius, the father of modern anatomy, was a famous man in his time. Born Andries van Wesel in 1514 in Brussels, he became the most important authority on anatomy of his time, daring even to correct the teachings of Galen, the ultimate reference on anatomy since the ancient times. Author of the most famous book on anatomy, the seven-volume "De Humani Corporis Fabrica, Libri Septem" , professor of surgery and anatomy in Padua at age 23 in 1537, imperial physician to the court of King Charles V and personal physician of the emperor of the Spanish Empire, King Philip II, Andreas Vesalius’ accomplishments are multifold. Yet, surprisingly, there are lots of things we do not know about him: how did he look like, for example, but also –and that is the topic of this paper- how did he die, what did he die from, and where exactly is he buried?
There have been more items related to Vesalius’ life that were wrongly transmitted through time, but recent investigations have put to rest a number of “disputed” facts that were erroneously reported and commonly accepted. They often made into the general history books or even into Wikipedia. The two most glaring ones were
1. That Andreas Vesalius had to leave the Imperial Court in Spain because the Inquisition was investigating him for allegedly doing an autopsy on a person that was not yet dead.
• We now know that Andreas Vesalius did not leave the Imperial Court for his pilgrimage to Jerusalem under pressure of the Inquisition, as is often alleged [1], but that he left on his own accord and with the full support of the Emperor who provided him with introduction letters to Spanish embassies abroad. We thought the Vesalius and the inquisition myth was laid to rest in 1928 [2], but has to be refuted again and again to this day, it seems [3].
2. That Andreas Vesalius was shipwrecked, and presumably drowned
• Vesalius did not die shipwrecked, as it was still alleged by Wikipedia recently [4] (but now corrected. His ship arrived safely at the harbour of the island of Venetian owned island of Zante (now Zakinthos, Greece) and Andreas Vesalius went ashore there.
What do we know for sure about the last days of Andreas Vesalius?
• We know that Andreas Vesalius undertook a pilgrimage to Jerusalem in early March 1564, arriving in Venice late April, and that he sailed from Venice via Cyprus to Jerusalem in early May. He only stayed for a short time in Jerusalem, probably one month. He then traveled from Jerusalem through the Sinai desert to Alexandria, Egypt and boarded a Venetian ship there in September 1564, heading for Venice.
• We know that the return journey was eventful. The ship was initially driven off course and then stuck without winds for over forty days which lead to food and water shortages on the ship. Most passengers fell ill, and many died. Their bodies were thrown overboard. This caused great anxiety to Andreas Vesalius who feared being thrown overboard unceremoniously in case he died. Vesalius became ill himself and lay sick in the hold with nobody taking care of him. (Account of Reinert Soleander, quoted by Biesbrouk et al.) [5].
• We also know that he stepped off the ship on the Venetian island of Zante (now Zakynthos in Greece) on October 15, 1564, sick, weak and frail, that he slowly walked towards the gates of the city where he collapsed and fell dead.
These are the facts that can be attested, and are not in dispute. What remains disputed is: did this 50 year old man die from scurvy, as is alleged?
In this article we will look at the arguments advanced in favour of the scurvy theory and see if there is any evidence to support these arguments.
Most arguments in favour of the scurvy theory have been proposed by Mr. Pavlos Plessas at the 2014 Vesalius Continuum meeting in Zakynthos, Greece and posted online on his blog (and here) [5]:
• “Vesalius stayed for six months in an area where Vitamin C was not easily found.
• Vesalius’s travels and sightseeing during the summer months means that some of his body’s Vitamin C reserves were lost through perspiration.
• Over the duration of his pilgrimage this could have exceeded 20% of his initial reserves. He then stayed an additional forty days at sea becoming vitamin C deficient.
• He reports Vesalius as immobile, depressed, with phobic and paranoid behavior,
• These can have sudden death syndrome upon restart of physical activity, which would also explain Vesalius' sudden death at the doors of the port of Zakynthos [7]..
Article continued here: Did Andreas Vesalius really die from scurvy? (2)
Sources:
1. https://circulatingnow.nlm.nih.gov/2014/10/15/the-death-of-andreas-vesalius/ accessed 27.12.2016
2. Matheson Cullen, G. Vesalius and the inquisition myth. Lancet, January 14, 1928, p 105-6.
3. Dirix Th. In search of Andreas Vesalius. The quest for the lost grave. Lannoo, 2014.
4. https://en.wikipedia.org/wiki/Andreas_Vesalius accessed on January 21, 2016
5. Biesbrouck M, Goddeeris Th, Steeno O. The last months of Andreas Vesalius. A coda. In Vesalius, Acta Internationalia Historiae Medicinae. 2012, 18 (No 2), 70-75.
6. Plessas P. http://www.parathemata.com/2014/09/pavlos-plessas-powerful-indications.html 2014. Accessed January 21, 2016.
7. https://www.clinicalanatomy.com/andreas-vesalius
Aa https://ods.od.nih.gov/factsheets/VitaminC-HealthProfessional/
8. Fain, O. La Revue de Médecine Interne, 2004; vol 25, Issue 12, 872-880.
9. Hodges RE, Hood J, Canham HE, Sauberlich HE, Baker EM. Clinical manifestations of ascorbic acid deficiency in man. Am J Clin Nutr 1971;24:432-43.
x. Hirschman JV, Raugi GJ. Adult scurvy. Journal of American Academy of Dermatology, 1999, 41; No 6, 895-909.
xx. Bartley W, Krebs HA, O’Brien JRP. Vitamin C requirement of human adults. Medical Research Council Special Report Series No 280. London: Her Majesty’s Stationary Office; 1953. P 1-179. Quoted in Hirschmann et al.
xxx Hodges RE, Baker EM, Hood J, Saueberlich HE, March SC. Experimental scurvy in man. American Journal of Clinical Nutrition. 1969;22:535-48.
10. Harrisons Principles of Internal Medicine, 1998; p 484-85
11. Leung FW, Guze PA: Adult scurvy. Annals of Emergency medicine; 1981; 10:652-655
12. Bennet M, Coninx R. The mystery of the wooden leg: vitamin C deficiency in East African prisons. Tropical Doctor, 2005; 35: 81-84.
13. Carpenter K. The history if scurvy and vitamin C.Cambridge University Press 1986, p29.
11. Bown S R. 4he Age of Scurvy. How a surgeon, a mariner and a gentleman helped Britain win the battle of Trafalgar. Summersdale, 2003, p 96-99.
15. Lind J. A treatise of the scurvy. Containing an inquiry into the nature, causes and cure of that disease. Together with a critical and chronological view of what has been published on the subject. Edinburgh: Sands, Murray and Cochran: 1753.
16. Kinsman RA, Hood J: Some behavioural effects of ascorbic acid deficiency. The American Journal of Clinical Nutrition, 1971, 455-464.
17. Biesbrouck M, Goddeeris Th, Steeno O: ‘Post Mortem’ Andreae Vesalii (1514 – 1564). Deel II. Het graf van Andreas Vesalius op Zakynthos. A. Vesalius, nr.4 December 2015. [in Dutch].
18. Bruce M Rothschild. Scurvy imaging. http://emedicine.medscape.com/article/413463-overview
- Details
- Written by: Prof. C. Uribe

Felix Fleischner, MD
One of the current challenges in medical sciences is to achieve a common and universal language that allows establishing, promoting the understanding and communication between people of different cultures and nationalities.
The use of anatomical and radiological terms in the chest is not exempt from this theme. An adequate terminology allows describing findings and unifying concepts that facilitate communication, teaching, research, in brief, the transmission of knowledge.
From the radiological point of view, ignorance of appropriate terminology creates confusion and may eventually lead to inaccuracies and misdiagnoses. Therefore, reaching consensus in terminology is an attempt to minimize the effects of language vices, which are unfortunately passed on to future generations.
On the other hand, in recent years, technical advances in radiology have improved the capture, recording and storage of images, which in turn has involved the need for a new language to explain new concepts.
Within this context, the Fleischner Society, an international and multidisciplinary medical society for thoracic radiology, was founded in 1969 in memory of Dr. Félix Fleischner. Among the objectives of this society is the publication of formal statements that have been adopted for several years, as standards in the field of chest radiology, generating an important point of discussion and consensus around this issue.
Thus, as in 1971 a proposal for initial terminology was made, which was consolidated in 1984 and 1996 with the publications of the Fleischner Society glossary for Chest X-rays and Tomographies respectively. In 2008 (Radiology 2008; 246: 697-722) this glossary is finally updated using new terms, modifying or eliminating some of those that have become obsolete and others in which their meaning has changed.
Sources:
1. Austin JHM, Müller NL, Friedman PJ. Glossary of Terms for CT of the Lungs: Recommendations of the Nomenclature Committee of The Fleischner Society. Radiology 1996; 200:327-30.
2. Fraser RS, Müller NL, Colman N, Pare PD. Diagnosis of diseases of the Chest. 4th ed. Philadelphia: WB Saunders Company, 1999.
3. Tuddenham WJ. Glossary of Terms for Thoracic Radiology: Recommendations of the Nomenclature Committee of The Fleischner Society. Am J Roentgenol 1984; 143:509-17.
4. Souza Jr AS, Araújo Neto CA, Jasinovodolinki D,Marchiori E, Kavakama J, Irion KL et al. Terminologia para a Descrição de Tomografia Computadorizada do Tórax (Sugestões Iniciais para um Consenso Brasileiro). Radiol Bras 2002; 35:125-8.
5.David M. Hansell, Alexander A. Bankier, Heber MacMahon, Theresa C. McLoud, Nestor L. Müller, and Jacques Remy Fleischner Society: Glossary of Terms for Thoracic Imaging Radiology 2008 246:3, 697-722
This article belongs to the series "Glossary of Terms for Thoracic Imaging" by Prof C. Uribe, MsC. This series is based on the "Glossary of Terms for Thoracic Imaging" by the Fleischner Society
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.

Johann Gottfried Zinn
Johann Gottfried Zinn (1727–1759) anatomist and botanist, was born on December 6, 1727 in the city of Ansbach, Germany. He started his medical studies in his native city, becoming later a student of Dr. Albrecht von Hallers at the University of Göttingen, and received his MD in 1749.
He left for Berlin to continue his studies but came back shortly thereafter. He became a professor of anatomy at the University of Göttingen and in 1753 he also became the director of the botanical garden in the same city.
He is known for his anatomical treatise on the anatomy of the human eye: “Descriptio anatomica oculi humani iconibus illustrata”. Because of this, his name has become an eponym in the “Zonule of Zinn”, a ring of strands that forms a fibrous band connecting the ciliary body with the capsule of the lens of the eye. Zonule of Zinn is sometimes referred to as the suspensory ligaments of the lens, or the “ligament of Zinn”. His name is also attached to the anular ring tendon found in the posterior aspect of the eye, the "anular tendon of Zinn". This ring serves as attachment for all the extraocular muscles of the eye and the optic nerve passes through the center of the ring.
Carol Linné (Carolus Linneaus) named a genus of flowers in the family Asteraceae known vernacularly today as “Zinnia” in his honor. Hover your cursor over his portrait to see the flower.
The chapter on orbital anatomy of his anatomy book, taken from the second edition in 1780, has been translated and the first of three parts is published in an issue of “Strabismus”
His book "Catalogus Plantarum Horti Academici Et Agri" can be read online here.
His life was short, dying at the early age of 32, but his name lives on in the name of a beautiful flower.
Sources:
1. “Johann Gottfried Zinn" Simonz, HJ Strabismus – 2004, Vol. 12, No.
2, p. 125 2. "Anatomical Description of the Human Eye" Zinn, JG Strabismus, 13:45–52, 2005
Images: Public Domain by Wikipedia Commons. 1. Own work I_am Jin, and H. Wilhem Dietz
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.

As part of the redesign of this website we added a sidebar called "A Moment in History". The objective is to create a series of articles to honor those individuals who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research. Later in the development of the series we became aware of other individuals who have contributed in different ways, but still added their life work to the advancement of medical knowledge, as is the case of Marcia Croker Noyes (1869-1946).
Who would not be moved by the work of Allesandra Gilliani (1307-1326), who is probably the first woman dissector in the history of Human Anatomy, with a tragic short life and a love story.
We also decided to add to this series Moments in History that have left a mark on health care, such as "The First Use of Anesthesia in Surgery", or the story of how many individuals and unknown, anonymous children helped to rid the Americas from the scourge of smallpox, in "The Balmis Expedition",
Another line of articles in this series are those that honor individuals who have used anatomical and surgical knowledge to further other areas of human knowledge, such as that of Juan Vucetich, who used the anatomical differences in fingerprints to create the science of dactiloscopy.
Yet another line of articles are those that are more personal and dear to the contributors of "Medical Terminology Daily", such as "The Ephraim McDowell House of Museum", or "Interesting Discovery in and Ex-Libris".
Recently, I had to work in the Wangensteen Historical Library researching rare and antique medical books. The highlight of this work was to be able to read books by authors whose names are attached as eponyms to anatomical landmarks (Ligament of Treitz, Hesselbach's Triangle), pathologies (Koplik's spots), surgical procedures (Billroth I and II), medical maneuvers (Heimlich maneuver), and surgical instruments (Finochietto retractor). Of course, the names given here are but a small sample of what has been written to date.
As of today this series is now searchable, all you have to do is type "A Moment in History" in our search page, click on the "A Moment in History" link at the top of the sidebar, or click here
The image in this article is that of Dr. Vaclav Treitz. His eponymically named Ligament of Treitz is the most read article in this blog.
Original image, public domain, courtesy of Wikipedia.org.
{kind=link}
- Details
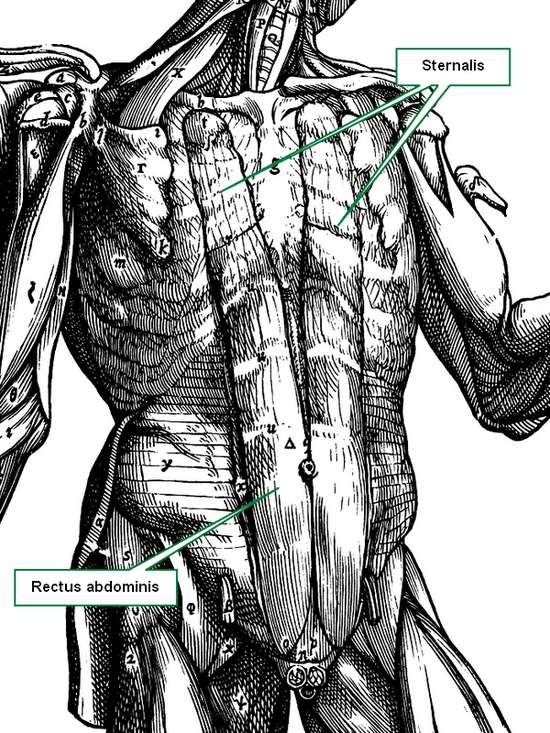
Sternalis muscle (Andreas Vesalius 1543)
The Sternalis muscle has been nominated as a supernumerary anatomical variation; the highest prevalence is in China (23.5%) and the lowest in Chile (0.87%).
The muscle is a wide band of muscular tissue located in the anterior thoracic wall, where fibers travel near-parallel to the sternum, inferior to the clavicles, aterior to the pectoralis major and the pectoral fascia. It has received many names: rectus sternalis, parasternal, episternal, superficial abdominal rectus, among other names. To avoid confusion, a true sternalis muscle should have the following characteristics:
(1) be localized between the subcutaneous tissue of the anterior thoracic region and fascia pectoralis;
(2) originate superiorly from the sternum or infraclavicular region;
(3) be inserted inferiorly in the ribs, rib cartilage, external oblique muscle aponeurosis and sheath of the rectus abdominis muscle;
(4) its innervation must come from the anterior root of the intercostal nerves. Another possible innervation from medial and lateral pectoral nerves has been mentioned.
Even though the Sternalis muscle does not appear to have a significant function, it is important to bear it in mind when evaluating mammograms, because one could misdiagnose it as a mammary cancer, as exposed by many authors. It is crucial to be familiar with this muscle to avoid confusion with pathology, such as extra-abdominal desmoid tumors, diabetic mastopathy, abscesses, hematomas, fat necrosis, and others; its unilateral presence may cause breast or chest asymmetry.
Note: The image in this article depicts this variation and is from the 1543 " De Humanis Corporis Fabrica, Libri Septem " by Andreas Vesalius.
Sources:
1. Jelev L., Georgiev G., Surchev L. (2001) The sternalis muscle in the Bulgarian population: classification of sternales. J. Anat. 199: 359-363.
2. Bradley F.M., Hoover H.C., Hulka C.A., Whitman G.J., McCarthy K.A., Hall D.A., Moore R., Kopans D.B. (1996) The sternalis muscle: an unusual normal finding seen on mammography. AJR. Am. J. Roentgenol. 166: 33-36.
3. Scott-Conner C.E.H., Al-Jurf A.S. (2002) The sternalis muscle. Clin. Anat. 15: 67-69.
4. Shiotani M., Higuchi T., Yoshimura N., Kiguchi T., Takahashi N., Maeda H., Aoyama H. (2012) The sternalis muscle: radiologic findings on MDCT. Jpn. J. Radiol. 30: 729-734.
- Details

Image property of: CAA.Inc.
WARNING: Depicts female external genitalia.
UPDATED: This article presents a case of vulvar hemangiomata. In superficial or surface anatomy, [vulva] is the anatomical name given to the external female genitalia.
The medical term [hemangioma] is formed by two root terms and a suffix. The root term [hem-] arises from the Greek word [αίμα] (a?ma) meaning "blood", the second root term [-angi-] .from the Greek term [αγγείο] (angeio), meaning "vessel” and the suffix [-oma] (ωμα), also Greek, meaning "mass", "growth”, or "tumor". The plural derivative word [hemangiomata] uses the suffix [-omata] which is the plural form of [-oma].
Vulvar hemangiomata are multiple blood growths or tumors on a female’s external genitalia. In most cases, hemangiomata are idiopathic.
Vulvar hemangiomata can be capillary (arterial) or cavernous (venous). They are benign vascular tumors which can be congenital, meaning the patient is born with them, or acquired, meaning that they appear later in life. In both cases they are usually asymptomatic. Patients may become concerned over aesthetics or because of bleeding due to trauma to the lesions. In rare cases, these hemangiomas can be large, requiring excision.
They are usually kept under observation, evaluating their progress (evolution or involution). If they increase in number or become symptomatic, intervention includes the use of sclerosing agents, destruction by cryotherapy or laser therapy, or surgical excision.
Personal note: My thanks to the patient who voluntarily and anonymously provided this image to further learning and knowledge on this pathology. Dr. Miranda